
The gender health gap represents a disparity in health outcomes and access to care between genders. This issue impacts individuals and broader societal well-being. Understanding this gap is a step toward fostering more equitable healthcare systems and improving overall population health. Addressing these differences requires a comperehensive approach. The unequal treatment within the healthcare system leads to serious consequences for patient health. A clear example is the delay in diagnosing conditions that predominantly affect one gender.
In this article, the definition of the gender health gap is provided, along with explanations of why it occurs, the delayed diagnosis of common diseases in women, and the lack of innovation in women's health research.
We have all probably heard about the gender pay gap and the gender gap in looking after household chores. But in this lecture, the much more important one will be discussed : Gender Gap in Innovation and Medical Research.
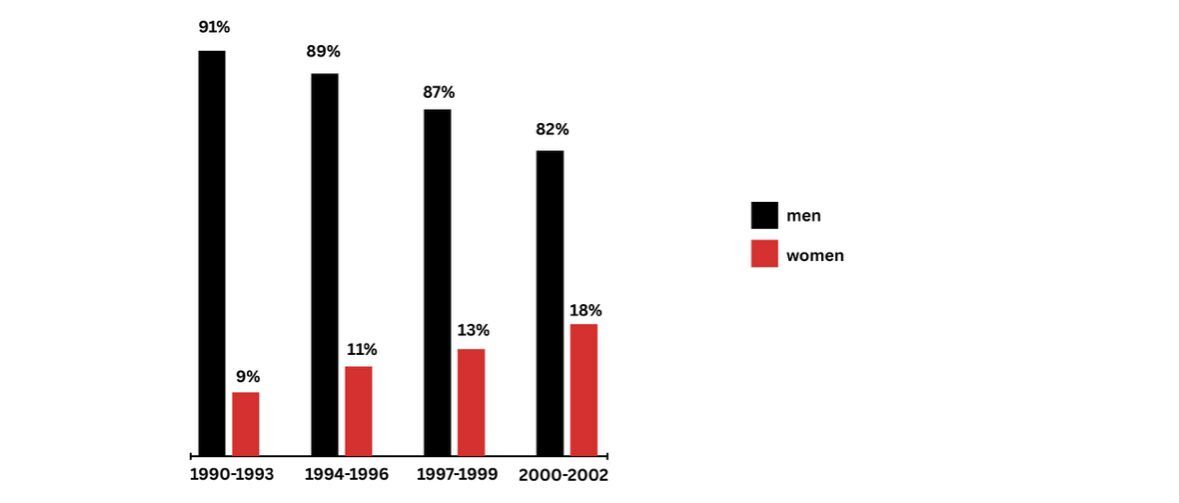
It was not untill 1993 that women first allowed to participate in clinical trials. It has been 33 years since women were first allowed to take part in modern medical research.
This means that majority of medications we use today like painkillers, sleep aids, anti-inflammatories were never designed for or tested on the female physiology. More shocking fact is that even medications that were designed specifically for women have not been tested on women.When take a look at adi the female viagra and of course it is in pink, it was approved after being tested in only 25 patients, 23 of which or 92 percent were men.
Such a massive gender gap in health care starts exceptionally early turns out that researchers not only prefer to have men in their clinical trials, they also prefer to have male mice over female mice in the early clinical studies.
Another really key example of the gender gap in health care is that it takes women a lot longer to get diagnosed with common diseases. The study that based on 7 million danish health records which were obtained over the course of 21 years and it shows that on avarege women get diagnosed later than men in over 700 different diseases. For cancer it takes four and a half years later to get a diagnosis and for diabetesit is two and half years more than men.This is really precious time that could be used to treat women instead of for them to wait for diagnosis.
Another gender gap in medical innovation is about period pain. 90% of women experience it. Yet no localized treatment has ever been developed. At the same time male conditions like erectile dysfunction which affect only 19% of men receive the lion share in clinical focus and research funding .While period pain might seem like an unimportant problem or a simple inconvenience, it is not and lack of innovation actually creates additional risks for the women who suffer from it. Midol is one of the most commonly prescribed medications. For the 90% of women that experience period pain, it turns out that it every month, you become dependent on it just as you can become dependent on opioid drugs. If you use them every month, they come with a number of severe side effects which come from the fact that painkillers were never designed for or tested on the female physiology. This lack of innovation exists despite the fact that researchers from University Collage London have discovered that period pain can be just as painful as having a heart attack.
Coronary diseases is leading cause of mortality in women. Women are 50% more likely to get misdiagnosed with a heart attack. It is because doctors are only trained to recognize the heart attack symptoms that appear in male physiology. As a result many women that show up to emergency rooms while having a heart attack get turned away and send home because doctors do not know how to recognize their symptoms.
Endometriosis is a condition that affects 1 in 10 women and it costs the british economy 2.4 billion eachb year. It takes 10 years to diagnose on avarege and it is not surprise that it takes so long because research into endometriosis is severly lacking. One of the largest studies in endometriosis ever it was not very helpful for patients at all. It looked at the correlation between how attractive a woman was perceived to be and how likely she was to have endometriosis. Result was like that: “Women with endometriosis were judged to be more attractive moreover they had a linear silhouette , larger breats and had sex for the first time at an earlier age”. How this data is useful for women with endometriosis is beyond us and yet this is a peer-reviwed published article.
The Speculum : An Ancienct Torture Device
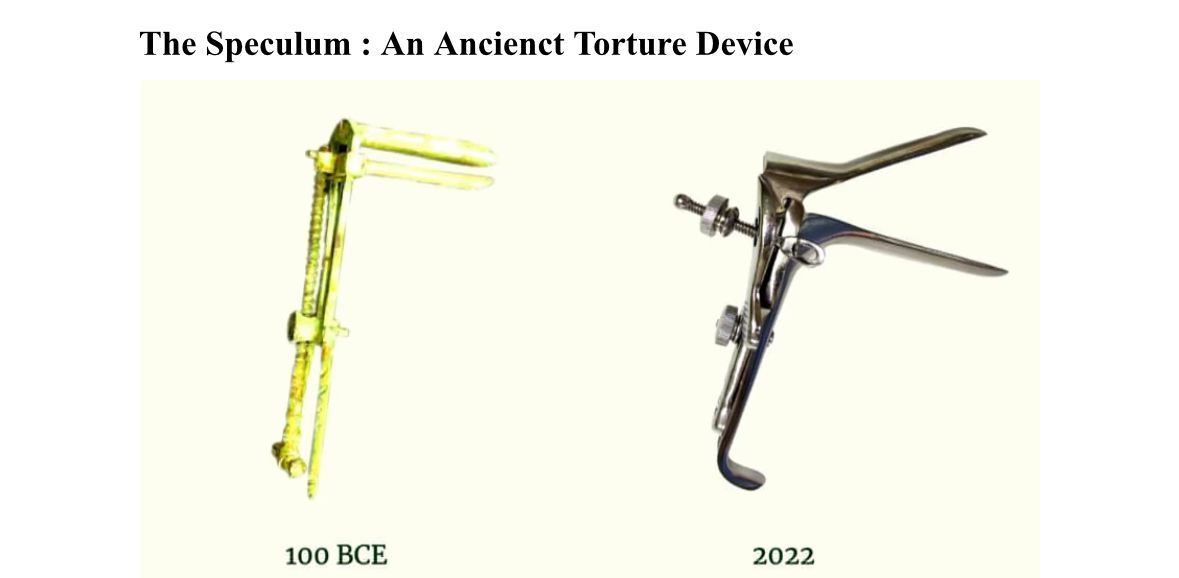
This is not a medieval torture device and it is not something really outdated that no one really uses anymore. This is in fact the central tool used in every gynecological exam today.It has the same design since it was first used in the roman empre. The speculum causes vaginal tearing and bleeding and it is quite painful to insert and remove.
References
- Shansky RM, Murphy AZ. Considering sex as a biological variable will require a global shift in science culture. Nature Neuroscience. 2021;24:457–464. doi:10.1038/s41593-021-00806-8
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. New England Journal of Medicine. 2020;383:2603–2615. doi:10.1056/NEJMoa2034577
- Dusenbery M. Doing Harm: The Truth About How Bad Medicine and Lazy Science Leave Women Dismissed, Misdiagnosed, and Sick. San Francisco: HarperOne; 2018
- Perez CC. Invisible Women: Data Bias in a World Designed for Men. New York: Abrams Press; 2019
- McGregor AJ. Sex Matters: How Male-Centric Medicine Endangers Women’s Health and What We Can Do About It. Paris: Hachette Go; 2020
- Beery AK, Zucker I. Sex bias in neuroscience and biomedical research. Neuroscience & Biobehavioral Reviews. 2011;35:565–572. doi:10.1016/j.neubiorev.2010.07.002
- Hay K, McDougal L, Percival V, Henry S, Klugman J, Wurie H. Disrupting gender norms in health systems: making the case for change. The Lancet. 2019;393:2535–2549. doi:10.1016/S0140-6736(19)30648-8
- Zucker I, Prendergast BJ. Sex differences in pharmacokinetics predict adverse drug reactions in women. Biology of Sex Differences. 2020;11:32











